Nina explores the physical manifestations that can be seen in patients due to nutritional insufficiencies

As dental professionals, we are in a fortunate position to notice changes in our patients over time. Therefore, as well as benefiting their oral health we can have a positive effect on their well-being.
In this article, the physical manifestations that can be seen in patients due to nutritional insufficiencies will be discussed so that you, the clinician, will have the confidence to action this when assessing and treating patients. The starting point of this article is in
the form of a case study.
Vitamin D
The thumb nails here belong to patient J.

J had been attending the surgery for routine care for years. At each appointment, I would notice the developmental issues on his thumb nails and suggest a visit to the GP for appropriate testing. Once it had been pointed out at a few appointments, the patient started to monitor them. They noticed that the condition of the thumb nails was declining, so an appointment was made with the GP.
The patient was referred by the GP for nail scraping and, with various blood tests, it was detected that they had a very low vitamin D status.
The patient had a history of skin cancer and after digging a little deeper it was found that they had avoided the sun at all costs due to the fear of getting skin cancer again. In fact, they were quite frightened at the prospect. The doctor advised that the deficiency had manifested this way due to the fact that vitamin D is necessary for the body to absorb calcium, which is needed to produce a healthy nail. The patient was told that this deficiency could have led to osteoporosis, as the same mechanism is needed for bone health. Sunyecz (2008) concluded that: ‘Vitamin D deficiency enhances the mobilization of calcium from the bone’ thus increasing the risk of osteoporosis.
This patient took a supplement as recommended by their doctor and levels are returning to normal. The patient now reports an increase in energy and a feeling of general well-being. They didn’t realize just how tired they were as how they felt had become their ‘normal’.
Vitamin D is well known for its role in general well-being, in particular inflammation and immunity. This was highlighted by a study by the University of Edinburgh in April 2019,
where researchers found the presence
of vitamin D ‘to affect key cells of the immune system’.
The reason patient J has been mentioned is because it highlights just how important noticing this development issue was for this patient.
How far could this deficiency have gone?
What potential impact would it have had
on their health?
It also gave me (as the clinician) an insight into what the patient had gone through in the past and how they still feel about it.
This helped towards creating a wonderful relationship between the two of us – one of empathy from myself and a feeling of really being cared for by the patient.
It also highlights the importance vitamin D can have when it comes to gum health and how deficiency could be a potential risk factor for periodontal disease.
Jagelaviciene et al (2018) concluded that: ‘Vitamin D is significant in periodontology’ due to the ‘specific immune response by suppressing the destructive effect of chronic periodontitis’ alongside the role in ’jawbone density homeostasis preventing osteoporosis’. Najeeb et al (2016) advised: ‘Clinical studies have suggested that a deficiency of vitamin D leads to periodontal inflammation and a delay in post-surgical periodontal healing’. Knowing this, could it be worth routinely liaising with GPs to have patients with periodontal disease have their vitamin D status checked?
If vitamin D deficiency is suspected then a
test is needed to provide a baseline before
supplementation is recommended.
Vitamin C
Vitamin C plays a huge role in the synthesis of collagen and the integrity of the blood vessels.
Insufficiency can manifest as small blood vessels in the floor of the mouth due to a lacking of the integrity of the blood vessels (Maxfield et al, 2019).
The history of the sailors in the 18th century
suffering from scurvy due to the absence of
vitamin c in their diet is well known. Scurvy is a condition that leads to ‘bleeding gums and loss of teeth’ (Maxfield et al, 2019).
The blood blisters may be more noticeable in
a patient who is a smoker as they use up a lot
more vitamin C due to the antioxidant properties it provides (Maxfield et al, 2019).

Reactive oxidative species (ROS) from leukocytes lead to the destruction of periodontal tissues when in the presence of bacteria (ie, plaque) and as they are non-specific, they will harm healthy tissues too. Najeeb and colleagues (2016) concluded in a systemic review of nutrition and periodontal health that: ‘Studies suggest that antioxidants may overcome the ROS-mediated inflammation of periodontal tissue’. With its role in collagen production and antioxidant properties, vitamin C is a very important nutrient for periodontal health.
According to the NHS website, an adult needs ‘40mg of vitamin C a day’, which can be easily achieved by eating a varied diet of fruit and vegetables. Ideally, advise your patient to eat 10 or 11 portions a day, while making them aware that vitamin C is water soluble and is therefore not stored in the body, as a result, it needs to be replenished daily.
Vitamin C is found in most fruits and vegetables, and Maxwell et al (2019) advise that ‘90% of vitamin C’ is absorbed this way. According to the National Institutes for Health (NIH), a smoker needs an additional 35mg per day, so may benefit from supplementation if they are not prepared to quit.
Magnesium
Insufficiency can manifest as tremor, tic, or twitching (DiNicolantinio et al, 2018), which can cause the tongue to quiver when at rest. This can be quite noticeable during dental treatment as it can move the instruments, or fight the suction tube when being retracted. Magnesium plays a vital role in the production of cellular energy, so if you notice a quivering tongue it wouldn’t cause any harm to recommend magnesium bath flakes, as magnesium is absorbed well transdermally. Kass et al (2017) in a pilot study found ‘a rise in magnesium serum in the urine of the participants’ after being treated with a transdermal application of magnesium. Cuciureanu and Vink (2011) provided a systematic review that concluded that ‘high stress levels are highly associated with magnesium levels’, meaning that when stressed we need more of this mineral. Goyal et al (2013) highlighted the link between stress with system inflammation including periodontal disease. This is due to the physical factors and also psychosocial behaviours linked with feeling highly stressed for example, poor oral hygiene, fatigue, etc. Food sources are numerous and include spinach, kale, broccoli, avocado, legumes such as kidney beans, and chickpeas, banana, raspberries, salmon, mackerel, and tuna.
Nina will be reviewing personal 1-2-1 food diary reviews during our retreat. Here's a link
B vitamins
B vitamins are sometimes known as ‘the stress vitamin’, as, like magnesium, we use up a lot more of these vitamins when stressed.
Young and colleagues (2019) provided a
systematic review that found an increase in B
vitamins either through diet or supplementation ‘improved mood’ and helped to ‘decrease anxiety in participants’.
If we don’t provide this additional need then
the following conditions can occur:
• Bi lateral sores in the corners of the mouth
can appear that don’t heal after a few weeks.

This can develop into angular cheilitis in the right environment
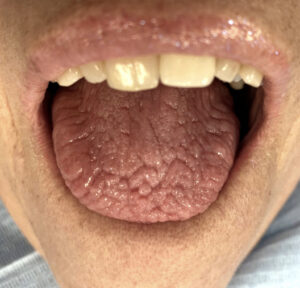
• Cracks in the tongue, red-tipped tongue and
geographic tongue can all be a sign that there
is a B vitamin deficiency/insufficiency.
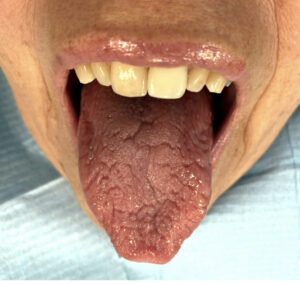
Glossitis also known as ‘red beefy tongue’
was described as ‘a useful tool to diagnosis B12 deficiency’ by Zhoul et al (2018).
They concluded that: ‘Physicians should pay special attention to oral manifestations during physical examination in high-risk populations such as the elderly, vegetarians, and patients with digestive problems.’
The study also advised that deficiency can lead to neurological problems later in life. While Miranti et al (2017) advised of the link between B vitamin deficiency and gastric cancer.
So, by noticing this and auctioning a GP referral, you could be potentially preventing a serious health issue in your patient. B vitamins are synthesized and absorbed in the small intestine, so if your patient has digestion/absorption issues, supplementation may not help them as they may struggle to absorb them and will only provide them with what my nutrition teacher explained in the classroom as ‘expensive urine. If the patient has digestive issues, they need to see their GP and/or nutritionist/dietician to help them with this. Supplementation may be needed in the form of an injection, which will bypass the digestive system.
The action to take here would be to refer to GP.
B vitamins can be found in most food sources, which include meats, seafood, dairies such as cheese and milk, dark leafy vegetables, beans, and legumes.
Essential fatty acids/omega 3
The National Institutes of Health describes the most common sign of deficiency as ‘rough, scaly skin and dermatitis’. This can be noticed as dry flaky lips or flaky skin under the eyes.
One of the reasons omega 3 is so important is because of the anti-inflammatory effect it has on the body.
However, in modern diets, a lot of our patients eat more omega-6 foods, usually processed foods rich in vegetable oils. This is problematic, as omega 6 has a pro-inflammatory effect on the body.
Hibbeln et al (2014) discussed the importance of the omega 3:6 ratio and if more omega 6 is consumed than omega 3 this ‘leads to a tilt toward inflammatory processes in the body’.
Simopoulos (2002) concluded in a literature
review that a beneficial ratio of 2/3 of
omega three to one on omega 6 suppresses
inflammation’
Recommend your patients eat oily fish two
or three times a week, while reducing foods
containing hydrogenated vegetable oils to help them to achieve this balance.
Zinc
According to Pisano and Hilas (2016): ‘Zinc
deficiency may lead to loss of appetite, impaired immune function, weight loss, delayed healing of wounds, eye and skin lesions, and smell and taste disturbances.
Even though there may not be a physical
manifestation present, a patient will often talk
about a bad taste or even lack of taste with the clinician.
Ozler et al (2014) advised that: ‘The findings
suggest a relationship with zinc deficiency and recurrent aphthous stomatitis’. Suggesting frequent oral ulceration could be connected to zinc deficiency.
Food sources include lamb, shellfish, nuts,
seeds, legumes, and eggs.
References are available on request.
Further Reading
Omega-3 fatty acids fact sheet,
from the National Institutes of Health,
Office of Dietary Supplements: ods.od.nih.
gov/factsheets/Omega3FattyAcids-
HealthProfessional
Vitamin C fact sheet, from the National
Institutes of Health, Office of Dietary
Supplements: ods.od.nih.gov/factsheets/
VitaminC-HealthProfessional
The Eatwell Guide from the NHS: www.nhs.
uk/live-well/eat-well/the-eatwell-guide
Take Home Messages
Always go from a food-first perspective and advise a wide and varied diet to avoid the deficiencies mentioned in this article. This includes:
• Oily fish two or three times a week,
while avoiding hydrogenated vegetable
fats to achieve an omega 3:6 ratio
• 10-11 portions of fruit and vegetables
a day
• 6-8 glasses of water per day.
• Do not supplement blindly as there may be
an underlying issue affecting absorption, green pharmacy can provide side effects
too and everyone has their own individual
needs, not to mention the risk of drug
interactions.
• The ability to use an inner detective when noticing conditions, are there a few symptoms combined which informs the clinician something about the patient?
For example, if a patient has a cracked
and quivering tongue this could highlight
that the patient is highly stressed or fatigued. Asking them how they are in themselves might mean they open up and give an insight as to what is affecting their motivation with routine.
• Refer to the appropriate person if the patient can benefit from this and they are open to it, it really does take a village when caring for patients and it is very important
to work within scope. Connect with people that can be referred to, to create an inner circle of like-minded people to provide the best care for the patient. This can be the
patient's GP, a local nutritionist/dietician, or any other healthcare professional that is relevant to the patient.
Originally published in Oral Health April 2021